Printable Flu Vaccine Consent Form Template
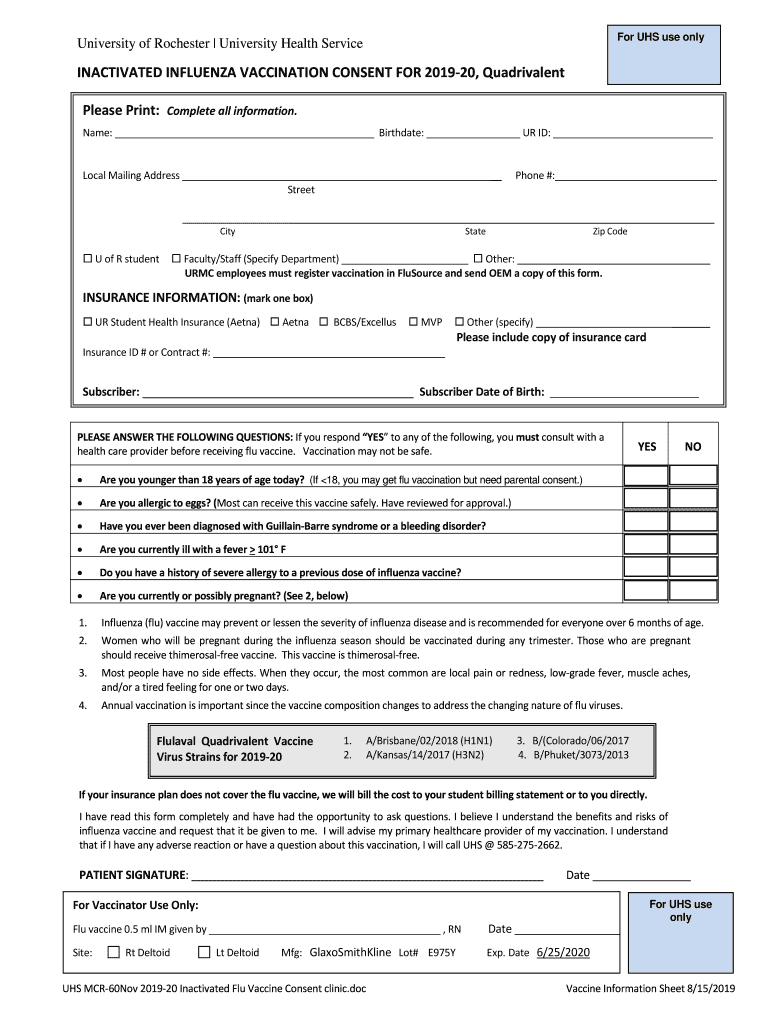
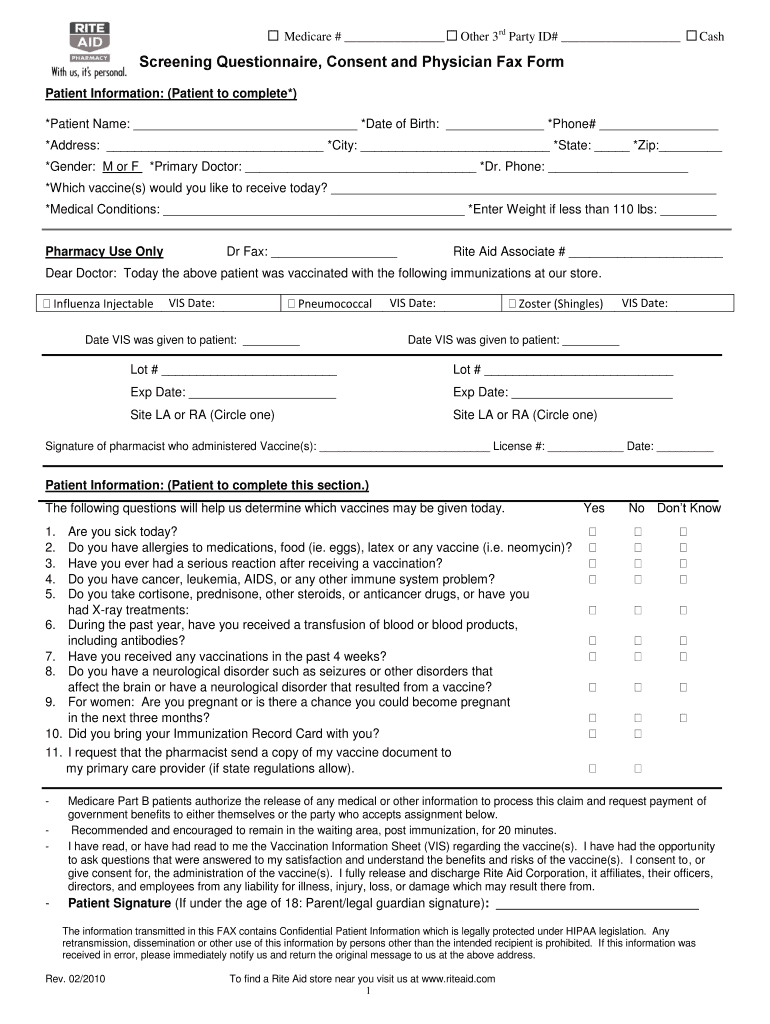
Printable Flu Vaccine Consent Form Template - Web first second if second, please indicate the date of the first dose: The cdc recommends annual flu vaccination as the first and. Centers for disease control and prevention, national. Annual influenza vaccine consent form. Web talk with your health care provider tell your vaccination provider if the person getting the vaccine: Has had an allergic reaction after. Web see the template consent forms: _____/______/____ (year, month, day) i consent to receiving.
Annual influenza vaccine consent form. Web first second if second, please indicate the date of the first dose: Has had an allergic reaction after. Centers for disease control and prevention, national. _____/______/____ (year, month, day) i consent to receiving. Web talk with your health care provider tell your vaccination provider if the person getting the vaccine: Web see the template consent forms: The cdc recommends annual flu vaccination as the first and.
_____/______/____ (year, month, day) i consent to receiving. Web see the template consent forms: Centers for disease control and prevention, national. Web first second if second, please indicate the date of the first dose: Annual influenza vaccine consent form. The cdc recommends annual flu vaccination as the first and. Has had an allergic reaction after. Web talk with your health care provider tell your vaccination provider if the person getting the vaccine:
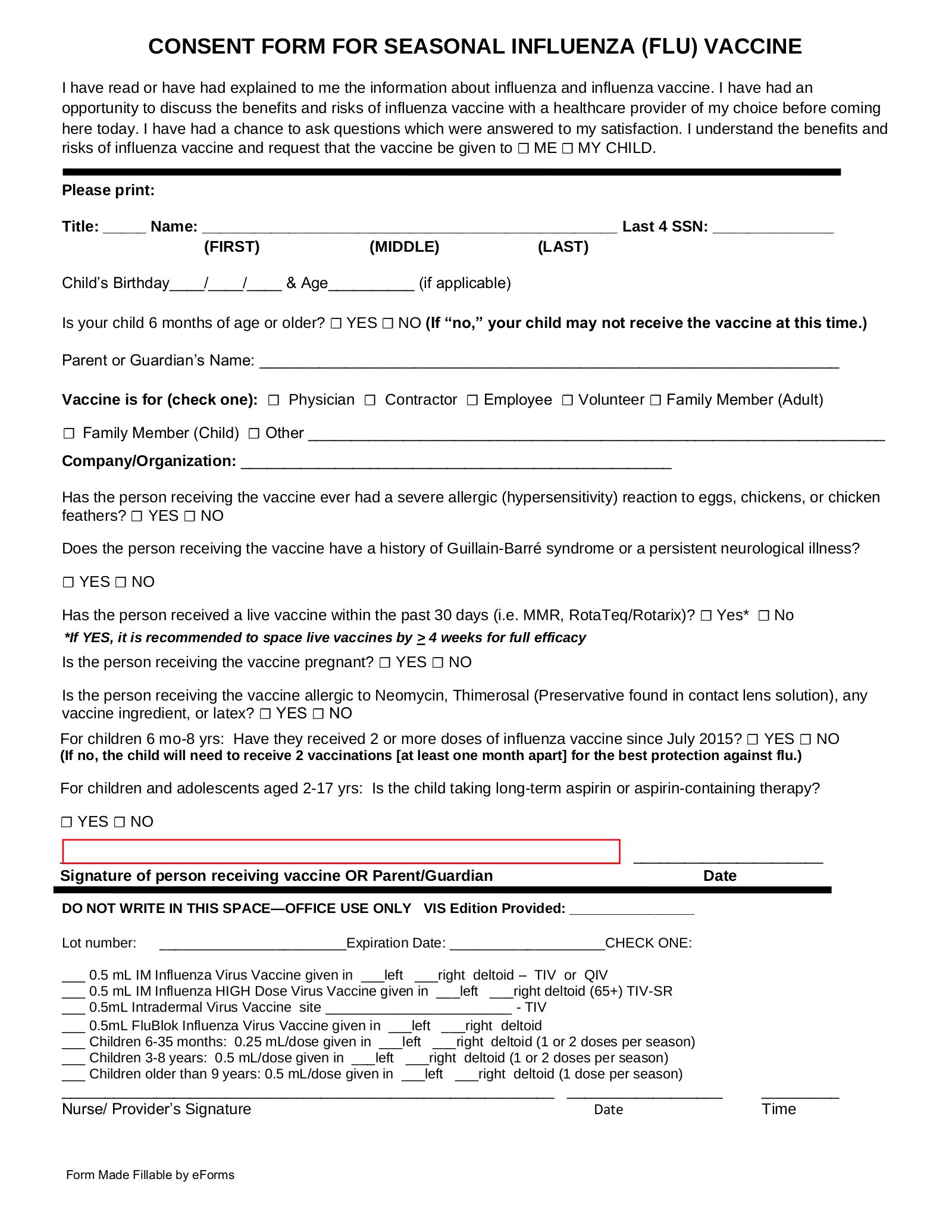
Free Flu Shot (Influenza) Vaccine Consent Form PDF Word eForms
Annual influenza vaccine consent form. Web see the template consent forms: _____/______/____ (year, month, day) i consent to receiving. The cdc recommends annual flu vaccination as the first and. Has had an allergic reaction after.

Printable Flu Vaccine Consent Form Printable Word Searches
Web talk with your health care provider tell your vaccination provider if the person getting the vaccine: The cdc recommends annual flu vaccination as the first and. Annual influenza vaccine consent form. Web first second if second, please indicate the date of the first dose: _____/______/____ (year, month, day) i consent to receiving.
Printable Flu Vaccine Consent Form Fill Out and Sign Printable PDF
Has had an allergic reaction after. Web talk with your health care provider tell your vaccination provider if the person getting the vaccine: _____/______/____ (year, month, day) i consent to receiving. Web see the template consent forms: Centers for disease control and prevention, national.
Vaccine Immunization Record 20182024 Form Fill Out and Sign
Web see the template consent forms: Annual influenza vaccine consent form. Has had an allergic reaction after. Web first second if second, please indicate the date of the first dose: The cdc recommends annual flu vaccination as the first and.
Walgreens Printable Proof Of Flu Shot Form
_____/______/____ (year, month, day) i consent to receiving. Web see the template consent forms: Web talk with your health care provider tell your vaccination provider if the person getting the vaccine: Annual influenza vaccine consent form. Web first second if second, please indicate the date of the first dose:
Printable Flu Vaccine Consent 20192023 Form Fill Out and Sign
The cdc recommends annual flu vaccination as the first and. Has had an allergic reaction after. Web first second if second, please indicate the date of the first dose: _____/______/____ (year, month, day) i consent to receiving. Web see the template consent forms:

Flu vaccine form Fill out & sign online DocHub
Annual influenza vaccine consent form. Centers for disease control and prevention, national. The cdc recommends annual flu vaccination as the first and. Web talk with your health care provider tell your vaccination provider if the person getting the vaccine: Web see the template consent forms:
Rite Aid Flu Shot 20122024 Form Fill Out and Sign Printable PDF
Web first second if second, please indicate the date of the first dose: Centers for disease control and prevention, national. _____/______/____ (year, month, day) i consent to receiving. Web talk with your health care provider tell your vaccination provider if the person getting the vaccine: Web see the template consent forms:

Hannaford flu shot Fill out & sign online DocHub
Web see the template consent forms: Annual influenza vaccine consent form. Web first second if second, please indicate the date of the first dose: Centers for disease control and prevention, national. Web talk with your health care provider tell your vaccination provider if the person getting the vaccine:

Flu Vaccination Consent Form 2 Free Templates in PDF, Word, Excel
Annual influenza vaccine consent form. Has had an allergic reaction after. Web talk with your health care provider tell your vaccination provider if the person getting the vaccine: Web first second if second, please indicate the date of the first dose: Web see the template consent forms:
Has Had An Allergic Reaction After.
Centers for disease control and prevention, national. _____/______/____ (year, month, day) i consent to receiving. Web talk with your health care provider tell your vaccination provider if the person getting the vaccine: Web see the template consent forms:
Web First Second If Second, Please Indicate The Date Of The First Dose:
Annual influenza vaccine consent form. The cdc recommends annual flu vaccination as the first and.